We all know providers are stressed for time and want to provide the best medical care to each and every one of their patients even in a short window of time. Unfortunately, the first thing to suffer is the documentation aspect of the visit. We’ve heard it before: “If it’s not documented, it didn’t happen.”
When we perform audits for our clients, the most common documentation errors we find are:
- Cloned notes. In this phenomenon, we discover that each progress note looks the same as the prior visit’s note, and the only thing that has changed is the patient’s vital signs. Cloned notes occur because most EMRs allow for copying/pasting or providers rely on click-boxes and templates. Cloned notes raise flags for regulators who then question the validity of other things on the progress note.
- Contradictions. The SOAP sections of the progress note should flow cohesively with each section contributing to the selection of diagnoses being assessed. When the exams (ROS/PE) don’t match what is documented in the assessment/plan, the resulting conditions must be questioned and cannot be coded (e.g., ROS says the patient denies numbness/tingling in the extremities, but the plan says, “Patient is experiencing/exhibiting numbness and tingling, and has neuropathy).
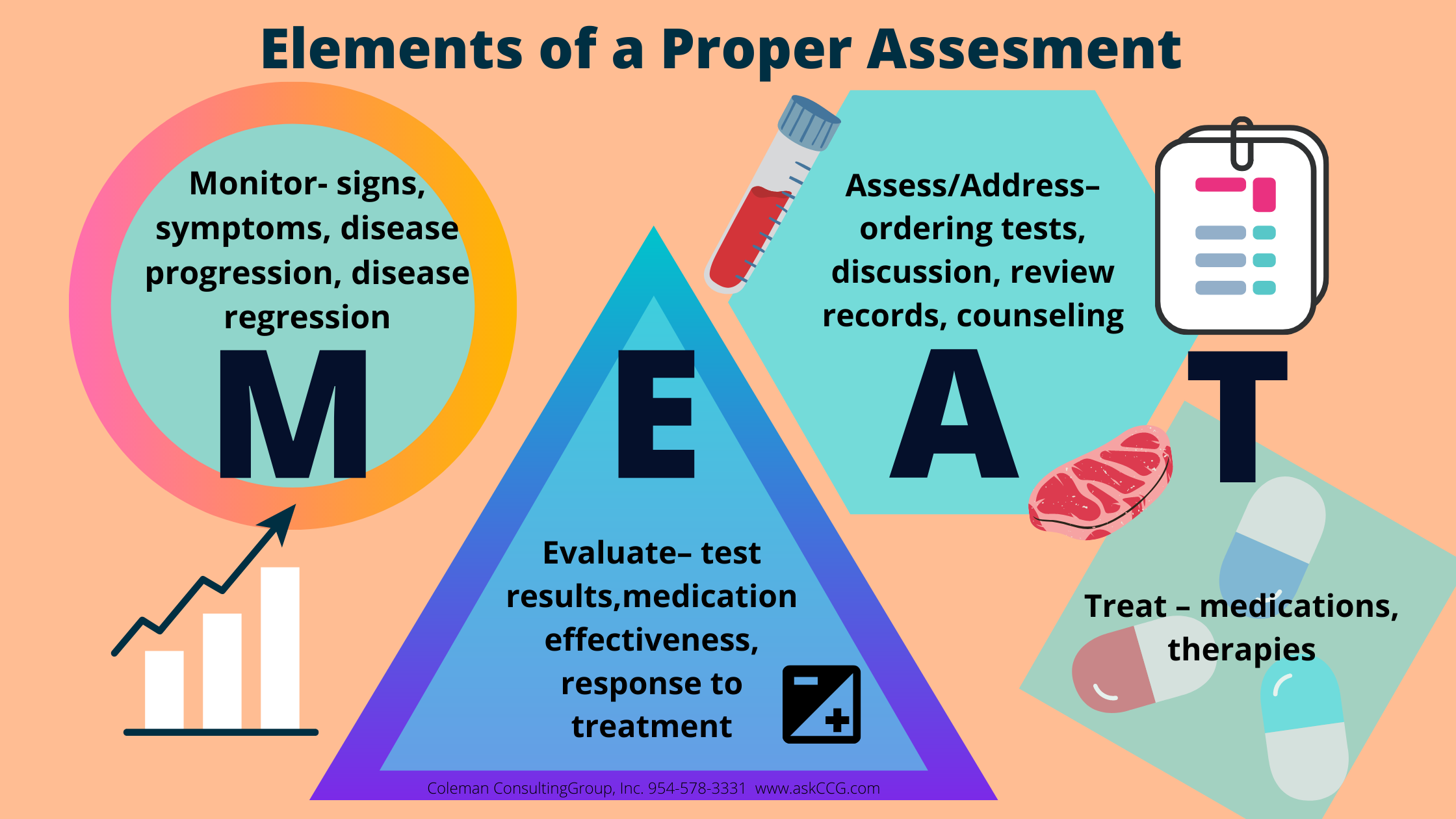
- No assessment of condition. The assessment must convey the status of the condition, how the patient is responding to treatment, and how the provider is managing the diagnosis. Simply ordering a test or refilling medications is not a sufficient assessment of a medical condition. Download our graphic to remind you of the proper elements of an assessment.
- Template verbiage. EMRs are a great tool in the medical practice but for every advantage, we can identify a concern. The convenience of pre-programmed templated language, such as “Stable, will continue to monitor” says very little about the condition and may prompt an auditor to disallow the condition because it wasn’t properly assessed. Read our blog on the Joys & Perils of Templates.
- Combination codes. ICD-10-CM created some welcome shortcuts where two linked conditions are reported with only one code. However, both conditions must be assessed. When, for example, Type 2 Diabetes Mellitus w/ polyneuropathy (E11.42) is reported, the provider must assess the diabetes and the polyneuropathy. If only one is assessed, the code cannot be validated.
{kind=link}
The progress note is a legal medical document and from an auditing standpoint, each one needs to stand alone and tell a story of the patient’s conditions. It’s important to consider that the usual PCP may not always be the one to see the patient and anyone who reviews the note should be able to quickly pick up the details of the patient’s care.